Locomoção
· A locomoção pode ser uma actividade voluntária ou automática

· É automática quando não é necrssário ter atenção
A locomoção é uma máquina complexa utilizando programas motores estereotipados, necessitando de:
· Alavancas – ossos e articulações
· Motor – músculos
· Energia – ATP
Marcha

http://www.scifa.univ-metz.fr/cours/Langlet/Locomotion.ppt#271,9,Diapositivo 9
É uma sucessão de passos, movimentos articulares simples de flexão e extensão
Fases da marcha
Há uma fase de apoio em que o pé está no chão e uma fase de oscilação em que está no ar

Para que movimento se realize torna-se necessário:
- · Apoio
- · Organização temporo-espacial
- · Regulação da tonicidade
- · Regulação do equilíbrio
Apoio
· Todos os corpos sofrem a acção da força da gravidade
· O centro de gravidade do corpo está na bacia, adiante da S2, numa linha passando pelos tetos dos acetábulos
· A reacção dos membros inferiores à gravidade é a contracção reflexa dos extensores
· Nos membros superiores, o apoio proximal é indispensável.É realizado através da inserção dos membros no tronco (espádua) e entre os segmentos dos membros
Organização temporo-espacial
· Para atingir a sua finalidade os deslocamentos dos membros devem ser organizados no espaço e no tempo.
· Esta regulação é efectuada pelo cérebro, tronco cerebral e cerebelo.
Regulação da tonicidade
· Para que o movimento se realize o tono muscular dos agonistas e antagonistas é regulado pelos centros subcorticais e pelo paleocerebelo e assegurado pelas vias motoras extrapiramidais
Regulação do equilíbrio
· A regulação correctiva do equilíbrio é assegurada pelos orgãos sensoriais visuais e vestibulares e pelos orgãos propioceptivos

Controle da locomoção
Tipos de movimentos
Quanto à capacidade em se moverem as articulações dividem-se em imóveis, pouco móveis e móveis
No quadro Seguinte estão indicados os principais tipos de movimentos
Principais tipos de movimentos
Adjusting angle between two parts
| Flexion - Bending movement that decreases the angle between two parts. Bending the elbow, or clenching a hand into a fist, are examples of flexion. When sitting down, the knees are flexed. Flexion of the hip or shoulder moves the limb forward (towards the anterior side of the body). | Extension - The opposite of flexion; a straightening movement that increases the angle between body parts. In a conventional handshake, the fingers are fully extended. When standing up, the knees are extended. Extension of the hip or shoulder moves the limb backward (towards the posterior side of the body). |
Adjusting relation to midline of body
| Abduction - A motion that pulls a structure or part away from the midline of the body (or, in the case of fingers and toes, spreading the digits apart, away from the centerline of the hand or foot). Abduction of the wrist is called radial deviation. Raising the arms laterally, to the sides, is an example of abduction. | Adduction - A motion that pulls a structure or part towards the midline of the body, or towards the midline of a limb. Dropping the arms to the sides, or bringing the knees together, are examples of adduction. In the case of the fingers or toes, adduction is closing the digits together. Adduction of the wrist is called ulnar deviation. |
Rotating body parts
| Internal rotation (or medial rotation) of the shoulder or hip would point the toes or the flexed forearm inwards (towards the midline). | External rotation (or lateral rotation) is the opposite. It would turn the toes or the flexed forearm outwards (away from the midline). |
Adjusting elevation
| Elevation - Movement in a superior direction. | Depression - Movement in an inferior direction, the opposite of elevation. -0 alex gale |
The movement of body [edit] General motion
Adjusting angle between two parts
| Flexion - Bending movement that decreases the angle between two parts. Bending the elbow, or clenching a hand into a fist, are examples of flexion. When sitting down, the knees are flexed. Flexion of the hip or shoulder moves the limb forward (towards the anterior side of the body). | Extension - The opposite of flexion; a straightening movement that increases the angle between body parts. In a conventional handshake, the fingers are fully extended. When standing up, the knees are extended. Extension of the hip or shoulder moves the limb backward (towards the posterior side of the body). |
Adjusting relation to midline of body
| Abduction - A motion that pulls a structure or part away from the midline of the body (or, in the case of fingers and toes, spreading the digits apart, away from the centerline of the hand or foot). Abduction of the wrist is called radial deviation. Raising the arms laterally, to the sides, is an example of abduction. | Adduction - A motion that pulls a structure or part towards the midline of the body, or towards the midline of a limb. Dropping the arms to the sides, or bringing the knees together, are examples of adduction. In the case of the fingers or toes, adduction is closing the digits together. Adduction of the wrist is called ulnar deviation. |
Rotating body parts
| Internal rotation (or medial rotation) of the shoulder or hip would point the toes or the flexed forearm inwards (towards the midline). | External rotation (or lateral rotation) is the opposite. It would turn the toes or the flexed forearm outwards (away from the midline). |
Adjusting elevation
| Elevation - Movement in a superior direction. | Depression - Movement in an inferior direction, the opposite of elevation. -0 alex gale |
[edit] Special motions of the hands and feet
surfaces of the hands and feet
|
The palm (adj palmar) of the hand corresponds to the sole (adj plantar) of the foot. The adjective volar, used mainly in orthopaedics, is synonymous with palmar and plantar.
|
The dorsum (back) of the hand corresponds to the dorsum (top) of the foot.
|
rotation of the forearm
|
Pronation - A rotation of the forearm that moves the palm from an anterior-facing position to a posterior-facing position, or palm facing down. This is not medial rotation as this must be performed when the arm is half flexed. (See also Pronator quadratus and Pronator teres muscle.)
|
Supination - The opposite of pronation, the rotation of the forearm so that the palm faces anteriorly, or palm facing up. The hand is supine (facing anteriorly) in the anatomical position. (See also Supinator muscle.)
|
flexion of the entire foot
|
Dorsiflexion - Flexion of the entire foot superiorly, as if taking one's foot off an automobile pedal.
|
Plantarflexion - Flexion of the entire foot inferiorly, as if pressing an automobile pedal. Occurs at ankle.
|
movement of the sole of the foot
|
Eversion - the movement of the sole of the foot away from the median plane.
|
Inversion - the movement of the sole towards the median plane (same as when an ankle is twisted
|
Deslizamento
· Passa-se nas articulações mais simples
· Uma superfície plana desloca-se sobre outra semelhante
· São exemplos os ossos do carpo e do tarso e os processos articulares da coluna
Flexão e extensão
Na flexão diminui o ângulo entre os ossos e na extensão diminui.
Para o conseguir na flexão uma parte no corpo é movida para diante e na extensão para trás excepto no joelho em que a flexão é para trás e a extensão para diante








Cortesia de George Murrell
Flexão e extensão
Hiperextensão
Extensão de uma articulação para lá do seu limite normal
Quando se tenta parar uma queda pondo uma mão à frente a força da queda cria uma hiperextensão do punho que pode levar a luxação ou fractura
Abdução e adução
1

cortesia de George Murrell
Dorsiflexão e flexão plantar
A flexão plantar é o movimento do pé para o lado plantar, como o pôr-se em bicos de pé

A dorsiflexão é o movimento dos pés na direcção da perna


Circundução
Combinação de vários movimentos - flexão, extensão, abdução e adução
Ocorre na articulação escápulo-umeral
O braço move-se de forma a descrever um cone com vértice no ombro
É o movimento feito pelos lançadores de basebol

http://www.brianmac.co.uk/musrom.htm
Rotação
· É o rodar de uma estrutura em torno do seu eixo mais longo - cabeça, úmero, anca e coxa, todo o corpo
· É o único movimento possível das duas primeiras cervicais



cortesia de George Murrell
Pronação e supinação
· Movimentos do rádio à volta do cúbito
· Na pronação a palma da mão roda de modo a que fique virada para trás e na supinação para a frente
·


Elevação e abaixamento
· A elevação move uma estrutura para cima, como a mandíbula ou a omoplata
· O abaixamento ou depressão move para baixo
Protracção e retracção
Na protracção ou propulsão a estrutura é movida para diante e na retracção ou retropulsão para trás

·
Oposição
· Movimento que permite que o polegar toque os outros dedos
Inversão e eversão
· Inversão é a rotação do tornozelo de modo a que superfície plantar do pé esteja virada para dentro ficando de frente para o pé do lado oposto
· A eversão é o movimento contrário, movendo-se o pé para o exterior
Amplitude do movimento
É o grau de mobilidade possível duma articulação
A amplitude de movimento activo é o movimento que se pode fazer pela contracção dos músculos que actuam sobre a articulação
A amplitude de movimento passivo é o movimento que se efectua quando as estruturas são movidas por uma força exterior como na fisioterapia
Vídeos sobre movimentos
BIBLIOGRAFIA
Directórios – movimento
Textos- movimento
Vídeos – movimentos
Anatomia do movimento
Fisiologia do movimento
Mecânica do movimento
Movimentos articulares
Visão durante o processo da marcha
FRACTURAS E LUXAÇÕES



Fractura por compressão




 http://radiographics.rsna.org/content/28/6/1755.full
http://radiographics.rsna.org/content/28/6/1755.full
























http://www.physio-pedia.com/Acromioclavicular_Joint

Movimentos do braço















FRACTURAS E LUXAÇÕES
Fracturas
Dá-se o nome de fractura quando um osso se partiu total ou parcialmente
Directorios
Textos
Natureza da fractura
Fractura aberta
Os topos dos ossos fracturados criam uma solução de continuidade nos tecidos moles e na pele, expondo o osso através da pele
Constitui um risco importante de infecção podendo provocar uma osteomielite
http://www.ortopaedi.dk/fileadmin/kurser/2014/Open_Fracture_nordic_plastic_surgery_course_2014.pdf
Fractura fechada
Não há solução de continuidade
Fractura incompleta (greenstick)
Os ossos não estão completamente separados
Frequente nas crianças
http://www.mayoclinic.org/diseases-conditions/greenstick-fractures/basics/definition/CON-20027302
Fractura transversal
.A fractura segue uma linha recta através do osso
Fractura obliqua
Fractura em espiral
Faz-se quando uma grande força faz rodar o osso sobre si próprio
Frequente nos desportistas
Fractura por compressão
Fractura cominutiva
Formaram-se mais de dois fragmentos
Fractura segmentar
Há fracturas multiplas de um ou dois ossos em que os segmentos se separam
Estes fracturas transformam-se facilmente em fracturas abertas
Fractura engrenada
Os fragmentos dos ossos encaixam-se uns nos outros
Fractura por avulsão
Um fragmento do osso separa-se da massa óssea principal
Pode dever-se à aplicação de forças externas ao tendão ou a uma forte contracção muscular
Fractura da placa de crescimento ou fractura de Salter- Harris
An X-ray of the left ankle showing a Salter–Harris type III fracture of medial malleolus. Black arrow demonstrates fracture line while the white arrow marks the growth plate.
Fracturas profissionais
Fracturas por stress
Prevenção e tratamento
Consolidação da fractura
Bone healing of a fracture by forming a callus as shown by X-ra
Etapas de consolidaçao das fracturas
Formação do calo cartilagíneo
Forma-se um tecido de granulação mole.
Os fibroblastos e os osteoblastos do periósteo e do endósteo vizinhos migram para o local da fractura.
Os fibroblastos formam fibras colagéneas que irão ligar os dois topos da fractura.
Certos fibroblastos diferenciam-se em condroblastos segregando uma matriz cartilagínea
No interior desta massa os osteoblastos começam a fazer osso esponjoso ao mesmo tempo que se forma uma massa cartilagínea que faz saliência para o exterior e acaba por se calcificar, formando-se assim o calo fibrocartilagíneo
Formação do calo ósseo
Os osteoblatos e osteoclastos continuam a migrar para o interior do calo fibrocartilagíneo, continuando a formar osso esponjoso, formando-se o calo ósseo.
Este processo inicia-se na terceira ou quarta semana ficando o osso completamente soldado três a quatro meses após o acidente
Remodelação óssea
Os materiais em excesso no exterior da diáfise e interior do canal medular são reabsorvidos e inicia-se a formação de osso compacto
Luxações e subluxações
Luxações
Deslocamento de um osso da sua posição normal na articulação Surge quando uma força extrema é aplicada num ligamento
Podem surgir quando de uma queda grave, sendo frequente nos desportistas particularmente nos desportos de contacto
São mais frequentes nas espáduas, dedos e polegares
As luxações de repetição são frequentes devido ao estiramento dos ligamentos e lassidão da cápsula
As luxações são pouco frequentes nas crianças jovens porque como as placas de crescimento são mais fracas que os músculos e tendões, têm mais tendência a responder com fracturas
Directorios
Textos
Subluxações
chiro.org/LINKS/ABSTRACTS/Does_VS_Exist.shtml
No seu conceito inicial subluxação resultava de uma vértebra ligeiramente mal alinhada mas não o suficiente para ser considerada uma luxação mas capaz de actuar sobre os nervos associados. Hoje aceita-se que há um compromisso neurológico.
Admite-se o seguinte modelo:
l perda de função das facetas articulares
l a articulação fica bloqueada
l Quanto a articulação fica bloqueada, os receptores da cápsula mandam sinais para o cérebro
l Como resposta, o cérebro envia sinais para que os músculos da articulação se contraiam para tentar libertar o bloqueio
l Quanto mais tempo durar o bloqueio, mais aumentará o tono muscular
Criticas
CINTURA ESCAPULAR
Ossos
Directorios
Textos gerais
A cintura escapular é constituída por dois ossos, a clavícula adiante e a omoplata
As duas cinturas escapulares e as omoplatas constituem as espáduas
As cinturas escapulares ligam os membros superiores ao esqueleto axial
Dão aos membros superiores uma flexibilidade e mobilidade única pelas seguintes razões:
Enquanto que a omoplata está ligada ao esqueleto, a omoplata pode-se mover livremente sobre o tórax e transferir esta mobilidade para os ossos
A cavidade articular da espádua ou cavidade glenoide é pouco profunda e mantida lassamente pelo que não dificulta os movimentos do úmero
CLAVICULAS
As clavículas são dois ossos longos em forma de S situadas na parte anterior e superior do tórax
Encontram-se imediatamente abaixo da pele, podendo-se palpar
https://en.wikipedia.org/wiki/Clavicle
OMOPLATAS
Ossos delgados, chatos e triangulares colocados na parte dorsal do tórax entre a 2º e a 7º costelas
Servem de fixação do membro superior ao tórax
Estão apoiadas sobre a zona superior e posterior da cavidade torácica e com elas se articulam a clavícula e o úmero
Tem 3 bordos – superior ou cervical, mediano ou espinal e lateral ou axilar
No bordo axilar encontra-se a cavidade glenoideia onde se articula com o úmero
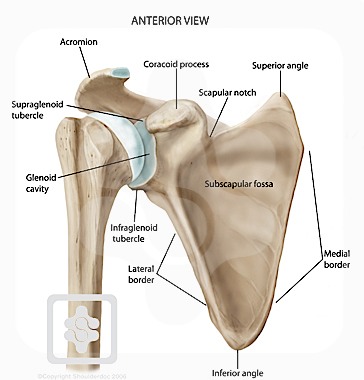
A face posterior da omoplata tem uma lamina transversal proeminente,a crista longitudinal ou espinha da omoplata que se termina num processo rugoso, o acromio que se articula com a extremidade acromial da clavícula
1. Subscapular fossa
2. Glenoid cavity
3. Coracoid process
4. Acromion
5. Superior border
6. Scapular notch
7. Superior angle
8. Medial border
9. Inferior angle
10. Lateral border
11. Infraglenoid tubercle
2. Glenoid cavity
3. Coracoid process
4. Acromion
5. Superior border
6. Scapular notch
7. Superior angle
8. Medial border
9. Inferior angle
10. Lateral border
11. Infraglenoid tubercle
{kind=link}
{kind=link}
{kind=link}
Articulações
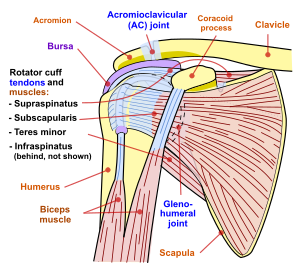
Para reduzir a fricção nos ligamentos existem varias bolsas
Articulação escapulo-humeral ou gleno-humeral
É a articulação mais móvel do organismo, tendo-se sacrificado a estabilidade pela mobilidade
É uma articulação esferóide
A cabeça do úmero insere-se na cavidade glenoideia da omoplata que é pequena e pouco profunda, representando apenas um terço da dimensão da cabeça do umero.
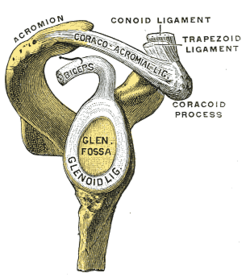
O bordo da cavidade glenoideia é ligeiramente ampliado por um anel fibrocartilagíneo, o debrum glenoideu
A cápsula articular muito laxa, conferindo à articulação uma grande liberdade de movimentos
Na face anterior os ligamentos coraco-umerais, gleno-umerais e transverso reforçam, ligeiramente a articulação. Os tendões musculares que atravessam a espádua contribuem fortemente para a sua estabilidade.
O mais importante é o tendão do bicípite
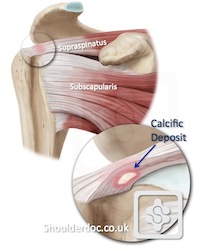
Coifa dos rotadores
Quatro tendões e músculos associados – subescapular, supra e infra-espinhoso e pequeno redondo – constituído a coifa dos rotadores ,fundem-se ao nível da cápsula e rodeiam a articulação Um movimento muito vigoroso de circundução , como no basebol produz um estiramento brutal dos quatro tendões
{kind=link}
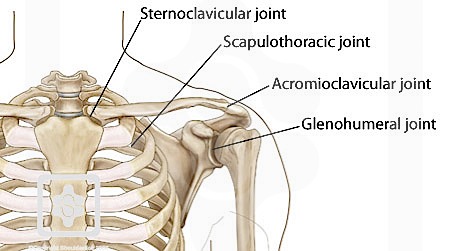
Outras articulações
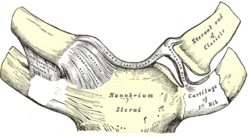
Esterno-clavicular
É uma articulação em sela com disco articular, multiaxial
http://www.instantanatomy.net/arm/joints/sternoclavicular.html
Acromioclavicular
Músculos da cintura escapular
Nove músculos cruzam a articulação para se inserirem no úmero. Todos partem da cintura escapular, excepto o grande dorsal e o grande peitoral
Só os músculos superficiais(grande peitoral, grande dorsal, deltóide) são agonistas dos movimentos do braço. Os outros são sinérgicos e fixadores.
Os supra e infra-espinhoso, o pequeno redondo e o infra-escapular são conhecidos como os músculos da coifa dos rotadores. Têm a sua origem na omoplata e os seus tendões dirigem-se para o úmero, confundindo-se com a cápsula fibrosa da articulação da espádua. Embora sejam sinérgicos dos movimentos angulares e circulares do braço a sua principal função é o reforço da cápsula articular.
Dum modo geral os músculos que nascem na parte anterior da articulação da espádua (grande peitoral, coraco-braquial e fibras da parte anterior do deltóide), assim como o bicípite, participam na flexão do braço
Os que nascem na parte posterior(grande dorsal, fibras posteriores do deltóide, grande redondo) participam na extensão
A abdução é efectuada pelo deltóide
No quadro seguinte iindicamos a origem, inserção, acção e enervação dos músculos da espádua
Name
|
Attachment
|
Function
|
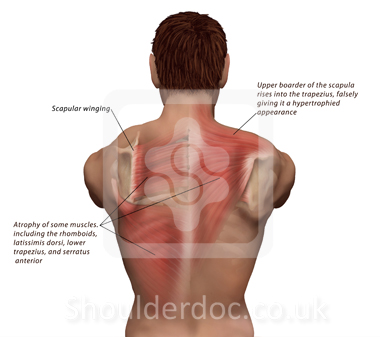
Originates on the surface of the upper eight ribs at the side of the chest and inserts along the entire anterior length of the medial border of the scapula.
|
It fixes the scapula into the thoracic wall and aids in rotation and abduction of the shoulders.[citation needed]
| |
Located inferior to the clavicle, originating on the first rib and inserting (penetrating) on the subclavian groove of the clavicle.
| ||
Arises from the third, fourth, and fifth ribs, near their cartilage and inserts into the medial border and upper surface of the coracoid process of the scapula.
|
This muscle aids in respiration, medially rotates the scapula, protracts the scapula, and also draws the scapula inferiorly.
| |
Attaches to the sternum (sterno-), the clavicle (cleido-), and the mastoid process of the temporal bone of the skull.
|
Most of its actions flex and rotate the head. In regards to the shoulder, however, it also aids in respiration by elevating the sternoclavicular joint when the head is fixed.[citation needed]
| |
Arises from the transverse processes of the first four cervical vertebrae and inserts into the medial border of the scapula.
| ||
They arise from the spinous processes of the thoracic vertebrae T1 to T5 as well as from the spinous processes of the seventh cervical. They insert on the medial border of the scapula, from about the level of the scapular spine to the scapula's inferior angle.
|
They are responsible for downward rotation of the scapula with the levator scapulae, as well as adduction of the scapula.
| |
Arises from the occipital bone, the ligamentum nuchae, the spinous process of the seventh cervical, and the spinous processes of all the thoracic vertebrae, and from the corresponding portion of the supraspinal ligament. It inserts on the lateral clavicle, the acromion process, and into the spine of the scapula.
|
Different portions of the fibers perform different actions on the scapula: depression, upward rotation, elevation, and adductions.[citation needed]
| |
deltoid, anterior fibers
|
The anterior fibres are involved in shoulder abduction when the shoulder is externally rotated. The anterior deltoid is weak in strict transverse flexion but assists the pectoralis major during shoulder transverse flexion / shoulder flexion (elbow slightly inferior to shoulders).
| |
deltoid, middle fibers
|
The middle fibres are involved in shoulder abduction when the shoulder is internally rotated, are involved in shoulder flexion when the shoulder is internally rotated, and are involved in shoulder transverse abduction (shoulder externally rotated) – but are not utilized significantly during strict transverse extension (shoulder internally rotated).[citation needed]
| |
deltoid, posterior fibers
|
Arises from the lower lip of the posterior border of the spine of the scapula, as far back as the triangular surface at its medial end.
|
The posterior fibres are strongly involved in transverse extension particularly since the latissimus dorsi muscle is very weak in strict transverse extension. The posterior deltoid is also the primary shoulder hyperextensor.
|
Os músculos que nascem na parte anterior da articulação( grande peitoral, coraco-braquial e fibras da parte anterior do deltóide efectuam a flexão do braço, acção em que também participa o bicípite.
Os músculos da parte posterior provocam a extensão( grande dorsal, fibras posteriores do deltóide, grande dorsal e grande redondo
Na abdução o deltóide é agonista e o grande dorsal é antagonista adiante e o grande dorsal atrás
Os músculos que agem sobre o úmero permitem a rotação lateral e mediana da espádua
PATOLOGIA DO OMBRO
Fracturas
As fracturas podem envolver a clavícula, colo do úmero e omoplata
A clavícula é o osso do organismo que mais se fractura
Há um ponto fraco a a 1/3 da extremidade externa. Nesta fractura a espádua o osso tende a descer
As fracturas da clavícula e do colo do úmero são provocadas em geral por quedas, colisões ou acidentes de automóvelComo a omoplata está protegida pelo tórax e músculos circundantes, a sua fractura é rara, podendo observar-se em acidentes de automovel, quase sempre associada a lesões do tórax
Fracturas da clavícula
Fractura da omoplata
Fractura do úmero proximal
Instabilidade da espadua
Luxações da espadua
As luxações são frequentes.
Como os tendões e ligamentos estão essencialmente nas regiões superior e anterior, nas luxações o úmero tem tendência a se deslocar para baixo
Como os principais ligamentos cruzam a face superior da articulação, é mais frequente a luxação inferior do úmero, na direcção da axila
A luxação acromio-clavicular é conhecida como espadua separada
A luxação esternoclavicular separa a clavícula do esterno
Na luxação glenohumeral a separação pode ser para diante ou para trás
Artrite acromioclavicular
Artrites da espadua
Bursites da espadua
A bursite infra-acromial pode tornar-se muito dolorosa quando o deltóide comprime a bolsa durante o movimento do ombro
Ombro congelado
A cápsula da articulação gleno-umeral inflama-se e torna-se rígida e forma adesões que limitam grandemente os movimentos da articulação.
Esta situação dura seis meses a mais de três anos
Muitas vezes a causa é desconhecida mas nalguns casos está associada a imobilização por fractura ou a traumatismos
Coifa dos rotadores
Rasgao dos rotadores
Debrum glenoideu
Rasgao do debrum
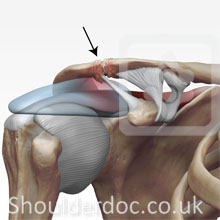
Depositos de cálcio na espadua
Dor no ombro
A dor no ombro pode dever-se a pressão da coifa dos rotadores ou a lesões dar ar ticulações gleno-umeral ou acromioclavicular. Todavia a maior parte das vezes provem de lesões do pescoço
Espadua alada
Espadua deslizante
http://www.moveforwardpt.com/symptomsconditionsdetail.aspx?cid=daafe3c4-da64-4f80-b01c-6a50ce1a290d
Exame da espadua
Osteolise da clavícula distal
Ruptura do bicipete no ombro
Separaçao do ombro
o the ligaments that hold your collarbone to your shoulder blade. In a mild separated shoulder, the ligaments may just be stretched. In severe injuries, ligaments may be completely ruptured.
In most people, a separated shoulder doesn't usually require surgery. Instead, conservative treatment — such as rest, ice and pain relievers — is often enough to relieve the pain. Most
http://radiopaedia.org/articles/acromioclavicular-inju
Sindroma de impacto do ombro ( impingement)
Impingement syndrome occurs when the rotator cuff tendons rub against the roof of the shoulder, the acromion.
In most parts of the body, the bones are surrounded by muscles. In the shoulder region, however, the muscle and tendons are surrounded by bone. If one taps on the top of the shoulder, bone can be felt immediately under the skin. Underneath that bone is the rotator cuff, a group of muscles and tendons that we use to lift the arm up overhead. The rotator cuff is sandwiched between the arm bone and the top of the shoulder (acromion). This unique arrangement of muscle and tendon between bone contributes to the development of impingement syndrome (shoulder bursitis, rotator cuff tendinitis).
When an injury to the rotator cuff occurs, it responds by swelling much the way an ankle does when it is sprained. However, because the rotator cuff is surrounded by bone, its swelling causes a number of events to occur. The pressure within the tendon increases, resulting in compression (squeezing) and loss of blood flow in the capillaries (small blood vessels).
When the blood flow is reduced, the tendon tissue begins to fray much like a rope. As the tissue swells, it results in the classic features of a pain like a toothache.
Tendinite do bicipete
Subscrever: Enviar comentários (Atom)
Sem comentários:
Enviar um comentário